Decoding the Human Spine: A Clinical Guide to Spinal Nerves
When patients enter a clinical practice describing radiating pain or unexplained numbness, the diagnostic journey frequently begins at the spine. The human nervous system operates as an intricate communication network. Studying a nerve chart back visualizes this web, mapping exactly where each structural root corresponds to physical sensation. Grasping this architecture remains crucial for both psychological comfort and physical health.
Individuals experiencing chronic discomfort often face significant psychological distress. Unpredictable bodily sensations can trigger anxiety, particularly when the underlying cause feels mysterious. By examining the structural layout of the peripheral nervous system, patients gain cognitive mastery over their symptoms. This knowledge transforms vague fears into actionable medical understanding.
What Are Spinal Nerves?
Spinal nerves are peripheral nerve bundles that transmit motor, sensory, and autonomic signals between the spinal cord and the rest of the body. There are thirty one pairs of these nerves in the human body. They function as bidirectional pathways for essential neurological communication, connecting the central nervous system to distant limbs and organs.
Every nerve root operates uniquely to keep the body functioning. Sensory fibers carry vital information like temperature or pain from the skin up to the brain. Simultaneously, motor fibers send commands from the brain down to the muscles to initiate movement. This constant exchange occurs within milliseconds, allowing for seamless environmental adaptation.
How to Read a Nerve Chart Back System
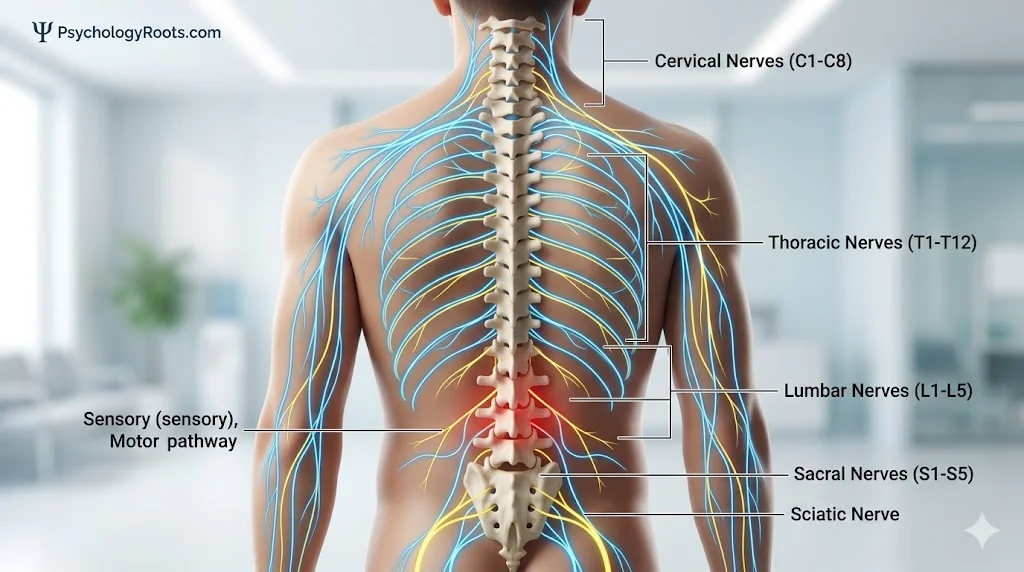
To comprehend these pathways, clinicians rely on precise anatomical mapping. A nerve chart visually divides the thirty one pairs of spinal nerves into distinct regional groups. These pairs emerge through small vertebral openings called intervertebral foramina. Each specific group corresponds to localized vertebrae and governs precise physiological territories.
The Cervical Nerves (C1 to C8)
Located in the neck region, the eight pairs of cervical nerves govern the upper extremities. These nerve roots control head movement, shoulder elevation, and arm mobility. The upper segment handles direct neck stability. The lower cervical roots form the brachial plexus, which directly dictates fine motor skills in the hands and fingers.
The Thoracic Nerves (T1 to T12)
The twelve pairs of thoracic nerves support the middle of the body. They extend outward into the chest cavity and abdominal muscles. These nerves play a critical structural role in maintaining posture and supporting respiratory mechanics. Sensory input from the ribcage and upper back relies entirely on the thoracic nerve network.
The Lumbar Nerves (L1 to L5)
Situated in the lower back, the five pairs of lumbar nerves bear significant mechanical stress. They govern the hips, the front of the thighs, and the knees. Because the lumbar region supports the majority of the body’s weight, these roots frequently become vulnerable to compression. This compression often leads to lower body mobility issues.
The Sacral Nerves (S1 to S5) and Coccygeal Nerve
The five pairs of sacral nerves manage pelvic function and the posterior segments of the legs. The prominent sacral plexus includes the sciatic nerve, which travels down the back of the thigh. Finally, the single pair of coccygeal nerves provides specialized sensory input to the skin directly surrounding the tailbone region.
How Do Spinal Nerves Function?
The functional reality of a spinal nerve begins at its dual roots. The dorsal root acts as the sensory intake valve, gathering data from the external environment. The ventral root serves as the motor output channel, driving muscular action. Together, they form a mixed spinal nerve capable of complex physiological regulation.
Psychologically, the perception of nerve signaling shapes human behavior. When a sensory nerve detects extreme heat, the pain signal forces an immediate withdrawal reflex. This is not merely a mechanical process. The brain registers the painful stimulus, encoding the experience into memory to prevent future tissue damage and promote evolutionary survival.
Autonomic functions also rely on these crucial spinal pathways. Involuntary processes like heart rate modulation, digestion, and glandular secretion depend on signals traveling through peripheral nerves. When stress activates the sympathetic nervous system, these pathways carry the fight or flight instructions that prepare the body for immediate action.
Common Causes of Spinal Nerve Damage
Spinal nerve damage frequently occurs due to mechanical compression. A herniated disc develops when the soft inner core of an intervertebral disc pushes through its tough exterior. This bulging tissue can impinge directly on adjacent nerve roots. Patients typically experience this as sharp, shooting pain traveling along the affected nerve pathway.
Trauma represents another frequent catalyst for neurological disruption. High impact events like falls or vehicle collisions can forcibly stretch or sever delicate nerve fibers. Neck injuries often compromise the cervical plexus, resulting in upper body weakness. Conversely, trauma to the lower back tends to disrupt the lumbar pathways, affecting leg stability.
Chronic nerve issues also stem from progressive medical conditions. Compressive neuropathy can develop gradually over years of repetitive physical strain. In rare instances, autoimmune disorders like Guillain-Barré syndrome actively attack the myelin sheath surrounding the nerves. This demyelination dramatically slows signal transmission, leading to profound muscle weakness and sensory deficits.
What Are the Clinical Treatment Options?
Addressing spinal nerve pathology requires a multifaceted clinical approach. Conservative management often begins with targeted physical therapy. Specialized exercises aim to relieve mechanical pressure on compromised nerve roots while strengthening surrounding supportive musculature. Clinicians frequently pair this physical rehabilitation with anti-inflammatory medications to reduce localized swelling and mitigate acute pain responses.
When structural compression becomes severe, surgical intervention may become necessary. Procedures like laminectomies or microdiscectomies remove the physical obstructions pressing against the neural pathways. Alongside physical treatments, psychological support remains highly beneficial. Cognitive behavioral therapy helps patients develop coping strategies for chronic pain, significantly improving their overall quality of life during recovery.
Living with persistent nerve pain requires patience and dedicated medical guidance. The human nervous system possesses a remarkable capacity for adaptation. While recovery timelines vary depending on the severity of the injury, understanding your anatomical structure is the vital first step. Consistent therapeutic engagement frequently yields substantial improvements in both mobility and daily comfort.
Key Takeaways
- There are thirty one pairs of spinal nerves facilitating communication between the brain and body.
- Nerves carry sensory, motor, and autonomic signals that regulate movement and environmental perception.
- Cervical nerves control the upper extremities, while lumbar and sacral nerves manage the lower body.
- Mechanical issues like herniated discs frequently cause localized pain by compressing adjacent nerve roots.
- Multidisciplinary treatment involving physical therapy and psychological support significantly improves patient recovery outcomes.
References
- Cleland, J. A., & Koppenhaver, S. (2015). Netter’s orthopaedic clinical examination: An evidence-based approach (3rd ed.). Elsevier.
- Kandel, E. R., Schwartz, J. H., Jessell, T. M., Siegelbaum, S. A., & Hudspeth, A. J. (2021). Principles of neural science (6th ed.). McGraw-Hill Education.
- Purves, D., Augustine, G. J., Fitzpatrick, D., Hall, W. C., LaMantia, A. S., & White, L. E. (2018). Neuroscience (6th ed.). Sinauer Associates.
- Ropper, A. H., Samuels, M. A., Klein, J. P., & Prasad, S. (2019). Adams and Victor’s principles of neurology (11th ed.). McGraw-Hill Education.
- Waxman, S. G. (2020). Clinical neuroanatomy (29th ed.). McGraw-Hill Education.